Name : Y.Navya sahithi reddy
Roll no:146
MBBS: 8TH SEMESTER
I have been given the following cases to solve in an attmept to understand the topic of 'Patient clinical data analysis' to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations, diagnosis and come up with a treatment plan.
This is the link to the questions asked regarding the cases:
http://medicinedepartment.blogspot.com/2021/05/online-blended-bimonthly-assignment.html?m=1
Below are my answers to the medicine assignment based on my comprehension of the case.
FIRST CASE: PULMONOLOGY
A 55-year-old female with shortness of breath, pedal edema, and facial puffiness.
https://soumyanadella128eloggm.blogspot.com/2021/05/a-55-year-old-female-with-shortness-of.html
question and answer
1) What is the evolution of the symptomatology in this patient in terms of an event timeline and where is the anatomical localization for the problem and what is the primary etiology of the patient's problem?
ans: EVOLUTION OF SYMTOMATOLOGY:first episode of SOB 20 years ago lasted for 1 week.
For the next 8 years, the patient has suffered from similar episodes of SOB every year.
12 years ago she had another episode of SOB. This one lasted 20 days.
For the past 12 years, she has been having yearly episodes and the latest episode, the SOB was of grade II
the latest episode of shortness of breath started 30 days ago.
2 days ago she started having SOB even at rest (grade IV).
diagnosed with diabetes 8 years ago.
5 years ago she was treated for anemia
1 month back she was experiencing generalized weakness.
Hypertension 20 days ago
pedal edema since 15 days
20 days ago due Covid 19 p showed signs of bronchiectasis.
Facial puffiness since 15 days.
On 4/5/21 she was started on empirical ATT.
drowsiness since 2 days
decreased urine output for the past 2 days.
using an indoor chulha for the past 20 years.
Operated for intestinal perforation 20 years ago
Cesarean section 21 years ago.
ANATOMICAL LOCALISATION OF THE PROBLEM: Lungs
Primary etiology of the patient problem: Usage of chuha for 20 years might be due to chronic usage.
2)what r the mechanism of action indication and efficacy over placebo of each of the phramacological and nonphramacological interventions used for this patient?
2Ans)Head end elevation :MOA
improves oxygenation
decreases incidence VAP
increases hemodynamic performance
increases end expiratory lung volume
decreases incidence of aspiration
#Indication:.head injury
.meningitis
.pneumonia
~ oxygen inhalation to maintain spo2
~Bipap:non invasive method
#MOA :assist ventilation by delivering positive expiratory and inspiratory pressure with out need for ET incubation.
3) What could be the causes for her current acute exacerbation?
ans. Cause for current acute excerbation - it could be due to any underlying infection.
4).could the ATT affected her symptoms if so how?
ans:Yes ATT affected her symptoms
Isoniazid and rifampcin -nephrotoxic - raised RFT was seen.
RFT:
Urea: 48 mg/dl
Creatinine: 1.9 mg/dl
Rifampicin-induced nephrotoxicity in a tuberculosis patient. Abstract. Rifampicin is a widely used anti-tuberculosis agent. On rare occasions, the drug can cause adverse effects such as acute renal failure, though most regain complete renal function upon discontinuation of therapy.
· The clinical use of nephrotoxic drugs in MDR-TB management may be unavoidable, so understanding mechanisms of their nephrotoxicity, early detection of drug-induced nephrotoxicity and reduction of the incidence of therapeutic side effects are important to avoid the end stage of renal failure
5.What could be the causes for her electrolyte imbalance?
ans :SERUM ELECTROLYTES:
18/5/21:
Na: 125 mEq/L
K: 3.5 mEq/L
Cl: 88 mEq/L
Water retention and hyponatraemia are typically observed in the final stages of Chronic Obstructive Pulmonary Disease (COPD) and the onset of edema is a poor prognostic factor. pathogenesis of edema in COPD patients was attributed to heart impairment because of pulmonary hypertension.
the pathogenesis of edema in these patients would be correlated with gas exchange impairment and in particular with carbon dioxide (CO2) retention. The gas exchange impairment induces, in these patients several hormonal abnormalities: renin (Rn), angiotensin II (AnII), aldosterone (Ald), atrial natriuretic peptide (ANP), vasopressin (ADH) and endothelial factors are some of the factors involved. The systemic response to hypercapnia has the effect of reducing the renal blood flow and, as a result, increasing water and sodium retention with the final effect of edema and hyponatraemia.
SECOND CASE: NEUROLOGY.
A)NEUROLOGY CASE 1
A 40 year old male with irrelevant talking
Link to patient details:
https://143vibhahegde.blogspot.com/2021/05/wernickes-encephalopathy.html
1) What is the evolution of the symptomatology in this patient in terms of an event timeline and where is the anatomical localization for the problem and what is the primary etiology of the patient's problem?
ans : evolution of symptomatology.
The patient was apparently asymptomatic 9 days ago, when he started talking, as well as laughing to himself,
a decrease in food intake since 9 days.
His last alcohol intake was on Monday, when he had drank around 1 bottle.
He also had short term memory loss since 9 days
he had 2-3 episodes of seizures, one being 1 year ago and the most recent being 4 months ago. The most recent time, (4 months ago), he had developed seizures
Following this episode, he started drinking again.
He was admitted to a tertiary care hospital on 15th May.
-History of 2-3 episodes of seizures in the last year, most likely due to alcohol consumption
Type 2 Diabetes since 2 years
Addicted to alcohol, drinks about 3-4 quarters per day- since 12 years
Addicted to cigarettes, smokes around 10 per day
anatomical localisation:Two important brain communication systems affected by alcohol involve the neurotransmitters:gamma-aminobutyric acid and glutamate.
primary etiology of the patient:
thiamine, one of the first B vitamins to be discovered also known as Vitamin B1, is a coenzyme that is essential for intricate organic pathways and plays a central role in cerebral metabolism. This vitamin acts as a cofactor for several enzymes in the Krebs cycle and the pentose phosphate pathway, including alpha-keto-glutamic acid oxidation and pyruvate decarboxylation. Thiamine-dependent enzymes function as a connection between glycolytic and citric acid cycles. Therefore, deficiency of thiamine will lead to decreased levels of alpha-keto-glutarate, acetate, citrate, acetylcholine and accumulation of lactate and pyruvate. This deficiency can cause metabolic imbalances leading to neurologic complications including neuronal cell death. Neuronal death in the mammillary bodies and thalamus were implicated in multiple cases of Wernicke encephalopathy studied. Studies involving computed tomography (CT) and magnetic resonance imaging (MRI) of patients with Wernicke encephalopathy revealed lesions in the thalamus with dilated ventricles and volume loss in the mammillary bodies. The lesions are usually symmetrical in the midbrain, hypothalamus, and cerebellum.
pathophysiology in this patient
The GABA system:GABA is an inhibitory neurotransmitter that helps to regulate brain function by rendering nerve cells less sensitive to further signaling. single doses of alcohol facilitate the inhibitory function of the GABA receptor, contributing to alcohol intoxicating effects. During withdrawal, brain GABA levels fall below normal and GABA activity declines. The combination of reduced brain GABA levels and GABAa receptor sensitivity may be contributed an adaptation to the presence of alcohol. In the absence of alcohol, the resulting decrease in inhibitory function may contribute to Symptoms of nervous system hyperactivity associated with both acute and protracted AW.
The glutamate system:The major excitatory neurotransmitter in the brain is glutamate, which communicates with three major subtypes of glutamate receptors. Among these, the N-methyl-D-aspartate (NMDA) receptor plays a role in memory, learning, and the generation of seizures. Alcohol inhibits the excitatory function of the NMDA receptor in laboratory studies at concentrations associated with mild to moderate alcohol intoxication in humans. As with the increased inhibitory function of the GABAA receptor, the decreased excitatory function of the NMDA receptor is consistent with alcohol’s general sedative effect. Long-term alcohol administration produces an adaptive increase in the function of NMDA receptors. Acute AW activates glutamate systems. In turn, AW seizures are associated with increased NMDA receptor function. Persistent alterations in NMDA receptor function may potentiate the neurotoxic and seizure-inducing effects of increased glutamate release during withdrawal.
The symptom: irrelevant talking, decreased food intake, tremors, sleep disturbance is due to the following reason: chronic alcohol consumption causes thiamine deficiency due to impaired absorption of thiamine from the intestine, a possible genetic predisposition, inadequate diet, reduced storage of thiamine in the liver and other nutritional deficient.
2) What are mechanism of action, indication and efficacy over placebo of each of the pharmacological and non pharmacological interventions used for this patient?
I) Thiamine helps the body cells change carbohydrates into energy. It has been used as a supplement to cope with thiamine deficiency
ii)Lorazepam binds to benzodiazepine receptors on the postsynaptic GABA-A ligand-gated chloride channel neuron at several sites within the central nervous system.it enhances the inhibitory effects of GABA, which increases the conductance of chloride ions into the cell
iii)pregabalin subtly reduces the synaptic release of several neurotransmitters, apparently by binding to alpha2-delta subunits, and possibly accounting for its actions invivo to reduce neuronal excitability and seizures.
iv)Lactulose is used in preventing and treating clinical portal-systemic encephalopathy .its chief mechanism of action is by decreasing the intestinal production and absorption of ammonia.
v)Potchlor liquid is used to treat low levels of potassium in the body.
Inj. 1amp THIAMINE in 100ml NS, TID.
Inj. Lorazepam
T. Pregabalin 75mg/PO/ BD
Lactulose 30ml/PO/BD
Syp Potchlor 10ml in one glass water/PO/BD
3) Why have neurological symptoms appeared this time, that were absent during withdrawal earlier? What could be a possible cause for this?
Due to excess thiamine deficiency
excess toxins accumulation due to renal disease caused by excess alcohol addiction.
4) What is the reason for giving thiamine in this patient?
ans: chronic alcohol consumption causes thiamine deficiency due to impaired absorption of thiamine from the intestine,Thiamine, one of the first B vitamins to be discovered also known as Vitamin B1, is a coenzyme that is essential for intricate organic pathways and plays a central role in cerebral metabolism. This vitamin acts as a cofactor for several enzymes in the Krebs cycle and the pentose phosphate pathway, including alpha-keto-glutamic acid oxidation and pyruvate decarboxylation. Thiamine-dependent enzymes function as a connection between glycolytic and citric acid cycles. Therefore, deficiency of thiamine will lead to decreased levels of alpha-keto-glutarate, acetate, citrate, acetylcholine, and accumulation of lactate and pyruvate. This deficiency can cause metabolic imbalances leading to neurologic complications including neuronal cell death.
5) What is the probable reason for kidney injury in this patient?
ans: The kidneys have an important job as a filter for harmful substances .alcohol causes changes in the function of the kidneys and makes them less able to filter the blood .alcohol also affects the ability to regulate fluid and electrolytes in the body. In addition, alcohol can disrupt hormones that disrupt hormones that affect kidney function .people who drink too much are more likely to have high blood pressure. High blood pressure is a common cause of kidney disease.
6). What is the probable cause for the normocytic anemia?
-Smear findings: Normocytic normochromic anemia, leukocytosis
alcohol causes iron deficiency or iron overload due its affect on production of new blood cells organs i.e,bonemarrow and the metabolism of iron
alocohol causes a affect on progenitor cells of blood causing decreased WBC ,RBC.
alochol decreases iron absorption from intestine .
7) Could chronic alcoholism have aggravated the foot ulcer formation? If yes, how and why?
ans:yes,As the patient is diabetic the chance of ulcer formation increases .in a patient of chronic alcoholic theimmune system is weak due to the affect on blood cells formation and iron absorption.due to this healing of an ulcer dampens.
B) NEUROLOGY CASE 2
A 52 year old male with cerebellar ataxia
Link to patient details:
1) What is the evolution of the symptomatology in this patient in terms of an event timeline and where is the anatomical localization for the problem and what is the primary etiology of the patient's problem?
ans:Timeline of the patient is as follows-
7 days back- Patient gave a history of giddiness that started around 7 in the morning; subsided upon taking rest; associated with one episode of vomiting
4 days back- Patient consumed alcohol; He developed giddiness that was sudden onset, continuous and gradually progressive. It increased on standing and while walking.
H/O postural instability- falls while walking
Associated with bilateral hearing loss, aural fullness, presence of tinnitus
Associated vomiting- 2-3 episodes per day, non projectile, non bilious without food particles
Present day of admission- Slurring of speech, deviation of mouth that got resolved the same day
Anatomical location- There is a presence of an infarct in the inferior cerebellar hemisphere of the brain
Etiology- Ataxia is the lack of muscle control or co-ordination of voluntary movements, such as walking or picking up objects. This is usually a result of damage to the cerebellum (part of the brain that controls muscle co-ordination)
Many conditions cause cerebellar ataxia- Head trauma, Alcohol abuse, certain medications eg. Barbituates, stroke, tumours, cerebral palsy, brain degeneration etc
.
In this case, the patient has hypertension for which he has been prescribed medication that he has not taken. Stroke due to an infarct can be caused by blockade or bleeding in the brain due to which blood supply to the brain is decreased, depriving it of essential oxygen and nutrients. This process could’ve caused the infarct formation in the cerebellar region of the brain, thus causing cerebellar ataxia.
2) What are the mechanism of action, indication and efficacy over placebo of each of the pharmacological and non pharmacological interventions used for this patient?
ANS.
A) Tab Vertin 8mg- This is betahistine, which is an anti- vertigo medication
MOA- It is a weak agonist on H1 receptors located on blood vessels of the inner ear. This leads to local vasodilation and increased vessel permeability. This can reverse the underlying problem.
Indications- Prescribed for balance disorders. In this case it is used due to patients history of giddiness and balance issues.
B) Tab Zofer 4mg- This is ondanseteron- It is an anti emetic
MOA- It is a 5H3 receptor antagonist on vagal afferents in the gut and they block receptors even in the CTZ and solitary tract nucleus
C) Tab Ecosprin 75mg- This is aspirin. It is an NSAID
MOA- They inhibit COX-1 and COX-2 thus decreasing the prostaglandin level and thromboxane synthesis
Indications- They are anti platelet medications and in this case used to prevent formation of blood clots in blood vessels and prevent stroke.
D)Tab Atorvostatin 40mg- This is a statin
MOA- It is an HMG CoA reductase inhibitor and thus inhibits the rate limiting step in cholesterol biosynthesis. It decreases blood LDL and VLDL, decreases cholesterol synthesis, thus increasing LDL receptors in liver and increasing LDL uptake and degeneration. Hence plasma LDL level decreases.
Indications- Used to treat primary hyperlipidemias. In this case it is used for primary prevention of stroke.
E) Clopidogrel 75mg- It is an antiplatelet medication
MOA- It inhibits ADP mediated platelet aggregation by blocking P2Y12 receptor on the platelets.
Indications- In this case it decreases the risk of heart disease and stroke by preventing clotting
F) Thiamine- It is vitamin B1
It is naturally found in many foods in the human diet. In this case, the patient consumes excess alcohol- so he may get thiamine deficiency due to poor nutrition and lack of essential vitamins due to impaired ability of the body to absorb these vitamins.
Indications- Given to this patient mainly to prevent Wernickes encephalopathy- that can lead to confusion, ataxia and opthalmoplegia.
G) Tab MVT- This is methylcobalamin
Mainly given in this case for vitamin B12 deficiency.
Tab Veratin 8 mg PO TID
Inj Zofer 4 mg IV/TID
Tab Ecosprin 75 mg PO/OD
Tab Atorvostatin 40 mg PO/HS
BP monitoring- 4rth hourly
Tab Clopidogrel 75 mg PO/OD
Inj Thiamine 1 AMP in 100 ml NSPO/BD
Tab MVT PO/OD
3) Did the patients history of denovo HTN contribute to his current condition?
A cerebellar infarct is usually caused by a blood clot obstructing blood flow to the cerebellum. High blood pressure that is seen in hypertension (especially if left untreated) can be a major risk factor for the formation of cerebellar infarcts.
Increased shear stress is caused on the blood vessels. The usual adaptive responses are impaired in this case, thus leading to endothelial dysfunction in this case. High BP can also promote cerebral small vessel disease. All these factors contribute to eventually lead to stroke.
4) Does the patients history of alcoholism make him more susceptible to ischaemic or haemorrhagic type of stroke?
ANS. Meta analysis of the relation between alcohol consumption and increased risk of stroke has mainly weighed in to the formation of two types- ischaemic and haemorrhagic stroke.
Ischaemic stroke- this is more common. This Is caused by a blood clot blocking the flow of blood and preventing oxygen from reaching the brain
Haemorrhagic stroke- occurs when an aneurysm bursts or when a weakened blood vessel leaks, thus causing cerebral haemorrhage
According to a Cambridge study, heavy drinkers have 1.6 more chance of intracerebral haemorrhage and a 1.8 increased chance of subaracnoid haemorrhage. The adverse effect on BP that is seen due to increased drinking is a major stroke risk factor and increase the risk of heart stroke.
Many studies show that with mild and moderate drinking . the risk of ischaemic stroke decreases due to decreased level of fibrinogen which helps in the formation of blood clots. However, heavy alcohol intake is associated with impaired fibrinolysis, increased platelet activation and increased BP and heart rate.
So In this case, his history of alcoholism, coupled with his hypertension definitely could be a causative factor of his current condition.
c) NEUROLOGY CASE 3
A 45 years old female patient with palpitations ,pedal edema, chest pain, chest heaviness ,radiating pain along the left upper limb
Link to patient details:
1) What is the evolution of the symptomatology in this patient in terms of an event timeline and where is the anatomical localization for the problem and what is the primary etiology of the patient's problem?
*She complains that she could feel her own heartbeat since 5 days and it is more rapid since yesterday night.
*Pain along her left upper limb associated with tingling and numbness-6 days
*Chestpain -since5 days
*Difficulty in breathing-5 days
*Swelling over the legs(bilateral)-8 months
8months back then she developed bilateral pedal edema
Palpitations: since 5days which are sudden in onset,more during night time
*dyspnoea during palpitations-since5 days
*Pain:since 6days radiating along the left upper limb which is dragging in nature
*Chest pain associated with chest heaviness
blood infection -7 months back
right and left)paresis due to hypokalemia 1year back
2 months back came to for treatment of neck pain for which she received medication
10 yrs back had the episode of paralysis of both upper and lowerlimbs(rt and left)
2) What are the reasons for recurrence of hypokalemia in her? Important risk factors for her hypokalemia?
Hypokalemic paralysis may lead to lethal cardiac dysrhythmia., , Therefore, early recognition and rapid correction of hypokalemia is essential. In our patient, the diagnostic dilemma was an acute onset of unilateral weakness,
3) What are the changes seen in ECG in case of hypokalemia and associated symptoms?
Increased P wave amplitudeProlongation of PR intervalWidespread ST depression and T wave flattening/inversionProminent U waves (best seen in the precordial leads V2-V3)Ecg:Apparent long QT interval due to fusion of T and U waves (= long QU interval)
D)NEUROLOGY CASE 4
55 YEAR OLD PATIENT WITH SEIZURES
Link to patient details:
1) Is there any relationship between occurrence of seizure to brain stroke. If yes what is the mechanism behind it?
seizures after ischaemic strokes. An increase in intracellular Ca2+ and Na+ with a resultant lower threshold for depolarisation, glutamate excitotoxicity, hypoxia, metabolic dysfunction, global hypoperfusion, and hyperperfusion injury
Seizures after haemorrhagic strokes are thought to be attributable to irritation due to (hemosideri. Deposits)caused by products of blood metabolism
Late onset seizures are associated with the persistent changes in neuronal excitability and gliotic scarring is most probably the underlying cause.
2. In the previous episodes of seizures, patient didn't loose his consciousness but in the recent episode he lost his consciousness what might be the reason?
Initially the patient might have had Simple partial seizures (no loss of consciousness) and might have progressed to Generalised Tonic Clonic seizures (loss of consciousness)
E) NEUROLOGY CASE 5
48 year old male with seizures and altered sensorium
Link to patient details:
1) What could have been the reason for this patient to develop ataxia in the past 1 year?
ans :an initial aura may be experincied by the patient depending on the cortical area from which the seizure orginates the patient then becomes rigid ,unconsious, falling heavily, risking facial injury .
cause may be due to addiction of alcohol
cerebral anoxia
2) What was the reason for his IC bleed? Does Alcoholism contribute to bleeding diatheses ?
Platelet function in alcoholic patients was assessed on admission and during abstinence in hospital. On admission platelets from these patients were significantly less responsive (percentage aggregation and thromboxane A2 release) to conventional in vitro aggregating agents (adrenaline, adenosine diphosphate, and collagen) than platelets from healthy, moderate drinkers. Initially, platelet counts in platelet rich plasma tended to be low and the Simplate II bleeding times frequently prolonged. Platelet aggregation and thromboxane A2 release, however, were inhibited even in patients with normal platelet counts on admission. Platelet aggregation and thromboxane A2 release returned to normal or became hyper-responsive during two to three weeks of abstinence. Platelet counts rose during this period, the largest responses occurring in those patients with the lowest counts on admission. Bleeding times reverted to normal during abstinence and correlated significantly with changes in platelet aggregation, thromboxane A2 release, and platelet count and with the estimated ethanol consumption during the week before admission. Chronic, heavy alcohol ingestion evidently exerts an inhibitory effect on platelet function even in the absence of alcohol in the blood, and this phenomenon is reversible on abstaining. The impaired platelet function, together with the reduced platelet count, may contribute to the bleeding diathesis associated with chronic alcoholism and to the increased incidence and it also responsible for intracranial haemmorhage'.
F) NEUROLOGY CASE 6
A 30 YEAR OLD MALE PATIENT WITH WEAKNESS OF RIGHT UPPER LIMB AND LOWER LIMB
1).Does the patient's history of road traffic accident have any role in his present condition?
:One cause of stroke after trauma is a tear in the head or neck blood vessels that lead to the brain, which can be a source of blood clots that cause a stroke. If a tear in these arteries can be diagnosed at the time of the trauma, a patient could be treated with an anti-clotting medicine to help prevent stroke.
2.What are warning signs of CVA?
. F - Face droopingOne side of the face drooping is a sign of a stroke. If part of the face is numb, that may also be a sign. To tell for sure, ask the person to smile. If the smile is lopsided, they may be having a stroke.
2. A - Arm weaknessAsk the person to lift both arms. If one arm is weaker and drifts down, they may be having a stroke. Numbness or weakness on one side of the body is a common stroke symptom.
3. S - SpeechSlurred speech or difficulty talking coherently may be a sign of stroke. Say a simple sentence like: "The sky is blue today." If the person has trouble repeating it, they may require medical attention.
4. T - TimeWhen someone is having a stroke, time is of the essence. If you suspect a stroke, get medical attention right away. Call 911 or take them to the nearest emergency department immediat
Weakness or numbness on one side of the body
Difficulty talking
Sudden changes in vision
Sudden difficulty walking
A sudden severe headache
Other signs of stroke include:
Confusion
Feeling dizzy
Lack of balance or stability
3.What is the drug rationale in CVA?
Aspirin -antiplatlet drug prevents stroke
Atorvostatin - decreases LDL cholesterol to prevent recurrent attacks of stroke
4. Does alcohol has any role in his attack?
ans : Excessive alcohol consumption has been associated with a wide range of medical conditions. Moderate alcohol consumption is linked to a lower risk of stroke than abstinence, whereas heavy alcohol consumption has been associated with an increased risk of stroke and stroke mortality. In addition to alcohol consumption, the most important risk factors for stroke are hypertension, coronary artery disease, cardiac insufficiency, atrial fibrillation, type 2 diabetes, smoking, overweight, asymptomatic carotid artery stenosis and elevated levels of cholesterol.
5.Does his lipid profile has any role for his attack??
Yes increased LDL causes atherosclerosis -Blood vessels - ischemia leads to - stroke
G) NEUROLOGY CASE 7
A 50 year old male patient with cervical myelopathy
Link to patient details:
1)What is myelopathy hand ?
There is loss of power of adduction and extension of the ulnar two or three fingers and an inability to grip and release rapidly with these fingers. These changes have been termed "myelopathy hand" and appear to be due to pyramidal tract involvement.
b)what is finger escape?
ans:Finger escape
Wartenberg's sign is a neurological sign consisting of involuntary abduction of the fifth (little) finger, caused by unopposed action of the extensor digiti minimi. . This finding of weak finger adduction in cervical myelopathy is also called the "finger escape sign".
c)what is Hoffman's sign?
ans:
Hoffman's sign or reflex is a test used to examine the reflexes of the upper extremities. This test is a quick, equipment-free way to test for the possible existence of spinal cord compression from a lesion on the spinal cord or another underlying nerve condition
H) NEUROLOGY CASE 8
A 17-year-old female with seizures.
1) What can be the cause of her condition?
the cause of her condition could be IRON DEFICIENCY ANEMIA.
2) What are the risk factors for cortical vein thrombosis?
Ans: Risk factors for children and infants include:
Problems with the way their blood forms clots
Sickle cell anemia
Chronic hemolytic anemia
Beta-thalassemia major
Heart disease — either congenital (you're born with it) or acquired (you develop it)
Iron deficiency
Certain infections
Dehydration
Head injury
For newborns, a mother who had certain infections or a history of infertility
Risk factors for adults include:
Pregnancy and the first few weeks after delivery
Problems with blood clotting; for example, antiphospholipid syndrome, protein C and S deficiency, antithrombin III deficiency, lupus anticoagulant, or factor V Leiden mutation
Cancer
Collagen vascular diseases like lupus, Wegener’s granulomatosis, and Behcet syndrome
Obesity
Low blood pressure in the brain (intracranial hypotension)
Inflammatory bowel diseases like Crohn’s disease or ulcerative colitis
3)There was a seizure-free period in between but again a sudden episode of GTCS why? resolved spontaneously why?
Ans: there was a seizure-free period due to the administration of antiepileptic drugs as the effect of drugs weans off the seizures appear again followed by administration of phenobarbitone leading to spontaneous resolution of the seizures.
4) What drug was used in suspicion of cortical venous sinus thrombosis?
Ans: heparin as CLEXANE was given to relieve clot in suspission of CVST
3) CARDIOLOGY
A)CARDIOLOGY CASE 1
A 78-year-old male with shortness of breath, chest pain, bilateral pedal edema, facial puffiness.
Link to patient details:
1.What is the difference between heart failure with preserved ejection fraction and with reduced ejection fraction?
Preserved ejection fraction (HFpEF) – also referred to as diastolic heart failure. The heart muscle contracts normally but the ventricles do not relax as they should during ventricular filling (or when the ventricles relax).
Reduced ejection fraction (HFrEF) – also referred to as systolic heart failure
HFpEF is preceded by chronic comorbidities, such as hypertension, type 2 diabetes mellitus (T2DM), obesity, and renal insufficiency, whereas HFrEF is often preceded by the acute or chronic loss of cardiomyocytes due to ischemia, a genetic mutation, myocarditis, or valvular disease
2.Why haven't we done pericardiocentesis in this patient?
Pericardiocentesis is not done here Because the effusion was self-healing, It reduced from 2.4cm to 1.9 cm.
3.What are the risk factors for the development of heart failure in the patient?
risk factors for the development of heart failure in this patent
Alcohol abuse increases the risk of atrial fibrillation, heart attack, and congestive heart failure
high blood pressure
Smoking
Diabetes
AV block can be associated with severe bradycardia and hemodynamic instability. It has a greater risk of progressing to third-degree (complete) heart block or asystole.
wosening of pericardial effusion leaing to cardiac tamponade.
4.What could be the cause for hypotension in this patient?
the visceral pericardium may have thickened which is restricting the heart to expand causing hypotension
(Maybe secondary to TB)
B) CARDIOLOGY CASE 2
A 70-year-old male patient with pedal edema,facial puffiness, and decreased urine output
Link to patient details:
1.What are the possible causes for heart failure in this patient?
the patient was a chronic alcoholic since 40yrs
type 2 diabetis mellitus
hypertension 19yrs
Pedal edema for 4 years associated with exertional dyspnea.
On checkup was diagnosed with CKD STAGE 4.
heavily built with central truncal obesity
The patient has elevated creatinine and AST/ALT ratios are>2 and was diagnosed with chronic kidney disease stage IV. CKD is also one of the risk factors for heart failure
these were the causes for heart failure in this patient.
2.what is the reason for anemia in this case?
ans:
The patient has normocytic normochromic anemia. it could be anemia of chronic disease as the patient is diagnosed with CKD stage IV.
Chronic kidney disease results in decreased production of erythropoietin which in turn decreases the production of red blood cells from the bone marrow.
Patients with anemia and CKD also tend to have a deficiency in nutrients like iron, vitamin B12, and folic acid essential in making healthy red blood cells.
3) What is the reason for blebs and non-healing ulcers in the legs of this patient?
ans:
The most common cause for blebs and non-healing ulcers in this patient is diabetes mellitus. CKD is also known to cause a delay in the healing of wounds along with poorly controlled diabetes. Anemia can also slow down the process of healing due to low oxygen levels.
4) What sequence of stages of diabetes has been noted in this patient?
ans:
There are 4 stages in type 2 diabetes- insulin resistance, prediabetes, type 2 diabetes, and type 2 diabetes and vascular complications, including retinopathy, nephropathy or neuropathy, and, or, related microvascular events.
The patient is diagnosed with diabetic Tripathy exhibiting a sequence of neuropathy, retinopathy, and nephropathy
The patient has been diagnosed with diabetic retinopathy, CKD stage IV, and shows signs of diabetic neuropathy such as numbness.
3) CARDIOLOGY CASE 3
A-FIB and BIATRIAL THROMBUS IN A 50-YEAR-OLD MALE PATIENT
Link to patient details:
1) What is the evolution of the symptomatology in this patient in terms of an event timeline and where is the anatomical localization for the problem and what is the primary etiology of the patient's problem?
ANS: Evolution of symptomatology
The patient was apparently asymptomatic 2 days ago when he developed Shortness of breath Grade II (on exertion) which progressed to Grade IV (at rest).
decreased urine output for 2 days and Anuria since morning
Shortness of breath (Grade II i.e SOB on exertion) 1yr ag
HTN since 1yr.
Facial puffiness On and Off since 2-3yrs.
surgery for hernia 10 years back
Off pain at surgical site which aggravated since 3yrs.
Constipation for 2 days
Occasional alcoholic, H/o NSAID abuse since 3yrs, non-smoker.
anatomical localization: cardiovascular system
primary etiology: Coronary heart disease, Hypertension, Valvular heart disease, Cardiomyopathy, Alcohol, Chest infection
2) What are the mechanism of action, indication, and efficacy over placebo of each of the pharmacological and non-pharmacological interventions used for this patient?
ans: Dobutamine MOA: acts on beta 1 receptor
Beta1 ionotropic effect → increases heart contractility → increases cardiac output
Indications are cardiogenic shock, Reversible heart failure
Digoxin MOA: Digoxin has two principal mechanisms of action which are selectively employed depending on the indication: Positive Ionotropic: It increases the force of contraction of the heart by reversibly inhibiting the activity of the myocardial Na-K ATPase pump, an enzyme that controls the movement of ions into the heart.
Indications are Atrial fibrillation, atrial flutter,
Heart failure, Abortion
3.What is the pathogenesis of renal involvement due to heart failure (cardiorenal syndrome)? Which type of cardiorenal syndrome is this patient?
Ans: Pathogenesis of cardiorenal syndrome is described below in the picture:
Stage 3 cardiorenal syndrome is seen in this patient
4. What are the risk factors for atherosclerosis in this patient?
Ans: Hypertension is the risk factor for atherosclerosis in this patient.
5. Why was the patient asked to get that APTT, INR tests for review?
And: Because of Thrombosis and to check on the development of thrombosis, this patient is asked to get APTT, INR tests for review.
4) CARDIOLOGY CASE 4
67-YEAR-OLD PATIENT WITH ACUTE CORONARY SYNDROME
D) Link to patient details:
1)What is the evolution of the symptomatology in this patient in terms of an event timeline and where is the anatomical localization for the problem and what is the primary etiology of the patient's problem?
ans:
TIMELINE OF EVENTS-
• Diabetes since 12 years - on medication
• Heartburn like episodes for a year- relieved without medication
• Diagnosed with pulmonary TB 7 months ago- completed the full course of treatment, presently sputum negative.
• Hypertension since 6 months - on medication
• Shortness of breath for half an hour-SOB even at rest
Anatomical localization - Cardiovascular system
Etiology: The patient is both Hypertensive and diabetic, both these conditions can cause
- Atherosclerosis: there is the build-up of fatty and fibrous material inside the wall of arteries.(PLAQUE)
2) What are the mechanism of action, indication, and efficacy over placebo of each of the pharmacological and non-pharmacological interventions used for this patient?
ans: Pharmacological interventions:
TAB MET XL 25 MG/STAT contains Metoprolol as the active ingredient
MOA: METOPROLOL is a cardioselective beta-blocker
Beta-blockers work by blocking the effects of the hormone epinephrine, also known as adrenaline. Beta-blockers cause your heart to beat more slowly( negative chronotropic effect)
and with less force( negative inotropic effect). Beta-blockers also help open up your veins and arteries to improve blood flow.
Indications: it is used to treat Angina, High blood pressure and to lower the risk of heart attacks.
EFFICACY STUDIES.
Patients were randomized to one of four treatment arms: placebo or ER metoprolol (0.2 mg/kg, 1.0 mg/kg, or 2.0 mg/kg). Data were analyzed on 140 intent-to-treat patients.
Results: mean baseline BP was 132/78 +/- 9/9 mmHg. Following 4 weeks of treatment, mean changes in sitting BP were: placebo = -1.9/-2.1 mmHg; ER metoprolol 0.2 mg/kg = -5.2/-3.1 mmHg; 1.0 mg/kg = -7.7/-4.9 mmHg; 2.0 mg/kg = -6.3/-7.5 mmHg. Compared with placebo, ER metoprolol significantly reduced systolic blood pressure (SBP) at the 1.0 and 2.0 mg/kg dose (P = .027 and P = .049, respectively), reduced diastolic blood pressure (DBP) at the 2.0 mg/kg dose (P = .017), and showed a statistically significant dose response relationship for the placebo-corrected change in DBP from baseline. There were no serious adverse events or adverse events requiring study drug discontinuation among patients receiving active therapy.
Non-pharmacological intervention advised to this patient is PERCUTANEOUS CORONARY INTERVENTION.
Percutaneous Coronary Intervention is a non-surgical procedure that uses a catheter (a thin flexible tube) to place a small structure called a stent to open up blood vessels in the heart that have been narrowed by plaque buildup ( atherosclerosis).
3) What are the indications and contraindications for PCI?
ans: INDICATIONS:
Acute ST-elevation myocardial infarction (STEMI)
Non–ST-elevation acute coronary syndrome (NSTE-ACS)
Unstable angina.
Stable angina.
Anginal equivalent (eg, dyspnea, arrhythmia, or dizziness, or syncope)
High-risk stress test findings.
CONTRAINDICATIONS:
Intolerance for oral antiplatelets long-term.
Absence of cardiac surgery backup.
Hypercoagulable state.
High-grade chronic kidney disease.
Chronic total occlusion of SVG.
An artery with a diameter of <1.5 mm.
4) What happens if a PCI is performed in a patient who does not need it? What are the harms of overtreatment and why is research on overtesting and overtreatment important to current healthcare systems?
ans:
Although PCI is generally a safe procedure, it might cause serious certain complications like
A)Bleeding
B) Blood vessel damage
C) Allergic reaction to the contrast dye used
D) Arrhythmias
E) Need for emergency coronary artery bypass grafting.
Because of all these complications, it is better to avoid PCI in patients who do not require it.
⁃ OVER-TESTING AND OVER-TREATMENT HAVE BECOME COMMON IN TODAY’S MEDICAL PRACTICE.
⁃ Research on overtesting and overtreatment is important as they are more harmful than useful.
Harms to patients
. Performing screening tests in patients who at low risk for the disease which is being screened.
For example, Breast Cancer Screenings Can Cause More Harm Than Good in Women Who Are at Low Risk. A harmless lump or bump could incorrectly come up as cancer during routine breast screenings. This means that some women undergo surgery, chemotherapy, or radiation for cancer that was never there in the first place
.
.Overuse of imaging techniques such as X- RAYS AND CT SCANS as a part of routine investigations.
Overuse of imaging can lead to a diagnosis of a condition that would have otherwise remained irrelevant - OVERDIAGNOSIS.
Also, the adverse effects due to this are more when compared to the benefits.
.Overdiagnosis through overtesting can psychologically harm the patient.
Hospitalizations[41] for those with chronic conditions who could be treated as outpatients[ can lead to economic burden and a feeling of isolation.
Harms to health care systems
The use of expensive technologies and machinery is causing a burden on health care systems.
5) CARDIOLOGY CASE 5
A 60-year-old patient with acute myocardial infarction
Link to patient details:
1) What is the evolution of the symptomatology in this patient in terms of an event timeline and where is the anatomical localization for the problem and what is the primary etiology of the patient's problem?
ans: Evolution of symptomatology
The patient was apparently asymptomatic 3 days back and then he developed mild chest pain in the right side of the chest.
The patient is a known case of hypertension and type 2 diabetes.
The patient took the first dose of COVISHEILD vaccine against COVID-19 5days back.
slightly disturbed for the past 3 days due to discomfort
*the anatomical location of etiology is BLOOD VESSELS.
myocardial infarction is usually due to thrombotic occlusion of a coronary vessel caused by the rupture of a vulnerable plaque. Ischemia induces profound metabolic and ionic perturbations in the affected myocardium and causes rapid depression of the systolic function
2) What are the mechanism of action, indication, and efficacy over placebo of each of the pharmacological and non-pharmacological interventions used for this patient?
Ans: PHARMACOLOGICAL INTERVENTION
1.TAB. ASPIRIN
mechanism: Aspirin inhibits platelet function through irreversible inhibition of cyclooxygenase (COX) activity. Until recently, aspirin has been mainly used for primary and secondary prevention of arterial antithrombotic events.
2.TAB ATORVAS
mechanism: Atorvastatin competitively inhibits 3-hydroxy-3-methylglutaryl-coenzyme A (HMG-CoA) reductase. By preventing the conversion of HMG-CoA to mevalonate, statin medications decrease cholesterol production in the liver.
3.TAB CLOPIBB
mechanism: The active metabolite of clopidogrel selectively inhibits the binding of adenosine diphosphate (ADP) to its platelet P2Y12 receptor and the subsequent ADP- mediated activation of the glycoprotein GPIIb/IIIa complex, thereby inhibiting platelet aggregation. This action is irreversible.
4.INJ HAI
mechanism: Regulates glucose metabolism
Insulin and its analogs lower blood glucose by stimulating peripheral glucose uptake, especially by skeletal muscle and fat, and by inhibiting hepatic glucose production; insulin inhibits lipolysis and proteolysis and enhances protein synthesis; targets include skeletal muscle, liver, and adipose tissue
5.ANGIOPLASTY
mechanism: Angioplasty, also known as balloon angioplasty and percutaneous transluminal angioplasty (PTA), is a minimally invasive endovascular procedure used to widen narrowed or obstructed arteries or veins, typically to treat arterial atherosclerosis.
3) Did the secondary PTCA do any good to the patient or was it unnecessary?
Ans: the second PCI was NOT necessary for this patient.
PCI performed from 3 to 28 days after MI does not decrease the incidence of death, reinfarction, or New York Heart Association (NYHA) class IV heart failure but it is associated with higher rates of both procedure-related and true ST elevation reinfarction.3 A retrospective analysis of the clinical data revealed The Thrombolysis in Myocardial Infarction (TIMI) Risk Score of 4 predicting 30-day mortality of 7.3% in this patient. Late PCI leads to the increased risks of periprocedural complications, long-term bleeding, and stent thrombosis.
The high incidence of CAD and the increasing need for PCI provide an opportunity to evaluate its appropriate use and highlight potential overuse. PCI is frequently reported to be overused and inappropriately recommended. Behnke et al defined overuse as ‘use of unnecessary care when alternatives may produce similar outcomes, resulting in a higher cost without increased value’.8Overuse causes a heavy financial burden on people living in countries, where fee-for-service and ill-regulated private healthcare provides much of the patient care. As a result, the cost of healthcare increases and causes potential harm to the patients.
6) CARDIOLOGY CASE 6
Link to patient details:
1. How did the patient get relieved from his shortness of breath after i.v fluids administration by a rural medical practitioner?
ANS: Because of the fluid loss that occurred to the patient
There is
Decreased preload → SOB occurred due to decreased cardiac output
IV fluids administered → there is an increase in preload → SOB decreased due to better cardiac output
2. What is the rationale for using torsemide in this patient?
Torsemide is used due to abdominal distension
3. Was the rationale for the administration of ceftriaxone? Was it prophylactic or for the treatment of UTI?
Treatment for UTI
Rationale - used for any bacterial infection
GASTROENTEROLOGY.
A) GASTROENTEROLOGY CASE 1
A 33 OLD MAN WITH PANCREATITIS, PESUDOCYST, LEFT BRONCHO PLEURAL FISTULA
Link to patient details:
1) What is the evolution of the symptomatology in this patient in terms of an event timeline and where is the anatomical localization for the problem and what is the primary etiology of the patient's problem?
ANS: Evolution of symptomatology
Patient was apparently asymptomatic 5 yrs back when he had painabdomen & vomitings
symptom free for nearly 3 yrs.
* Later he again started taking alcohol following which he had recurrent episodes of pain abdomen & vomiting
* (5-6 episodes in the past 1 year)
* From the past 20 days he had increased amount alcohol consumption (5 bottles of toddy per day)
* Last binge of alcohol 1 week back following which he again had pain abdomen & vomiting from 1 week and fever from 4 days.
* abdominal pain in umbilical, left hypochondriac, left lumbar and hypogastric regions.
* Abdominal pain was incresed after food intake.
* Pain is throbbing type and radiating to back and is associated with nausea and vomiting( 1 episode) , which is non bilious, non projectile and also has food particles and water content 1 week.
* Fever was high grade, continuous and associated with chills and vomiting
* Then he developed constipation since 4 days and passing flatus.
* patient also had burning micturition since 4 days, which is associated with suprapubic pain, increased frequency and urgency
*anatomical location of etiology is pancreas(ductal obstruction, acinar cell injury, defective intracellular transport)
*The pathophysiology of acute pancreatitis is characterized by a loss of intracellular and extracellular compartmentation, by an obstruction of pancreatic secretory transport, and by activation of pancreatic enzymes Attributed to alcohol
Consumed 3 sara bottles per day for 5 yrs and then stopped for 3 yrs and again started drinking from last 1 yr which increased to 5 bottles per day from past 20 days.
2) khaini : 1 per day since 5 yrs.
3) Ghutka: 5 per day since 6 months.
*antomical location of etiology is pancreas(ductal obstruction,acinar cell injury,defective intracellular transport)
*The pathophysiology of acute pancreatitis is characterized by a loss of intracellular and extracellular compartmentation, by an obstruction of pancreatic secretory transport and by an activation of pancreatic enzymes Attributed to alcohol
2) What is the efficacy of drugs used along with other non pharmacological treatment modalities and how would you approach this patient as a treating physician?
Ans:
PHARMACOLOGICAL INTERVENTIONS
1) ING. MEROPENAM
mechanism:Meropenem is bactericidal except against Listeria monocytogenes, where it is bacteriostatic. It inhibits bacterial cell wall synthesis like other β-lactam antibiotics. In contrast to other beta-lactams, it is highly resistant to degradation by β-lactamases or cephalosporinases.
P2) ING. METROGYL
mechanism:Metronidazole diffuses into the organism, inhibits protein synthesis by interacting with DNA and causing a loss of helical DNA structure and strand breakage. Therefore, it causes cell death in susceptible organisms.
3) ING. AMIKACIN
mechanism:he primary mechanism of action of amikacin is the same as that for all aminoglycosides. It binds to bacterial 30S ribosomal subunits and interferes with mRNA binding and tRNA acceptor sites, interfering with bacterial growth.
4) TPN ( Total Parenteral Nutrition )
mechanism: the early administration of enteral nutrition must be the standard therapeutic approach in patients with severe acute pancreatitis it decreases the risk of infection; TPN is only required in a few patients.
5) IV NS / RL
mechanism:Patients with acute pancreatitis lose a large amount of fluids to third spacing into the retroperitoneum and intra-abdominal areas. Accordingly, they require prompt intravenous (IV) hydration within the first 24 hours. Especially in the early phase of the illness, aggressive fluid resuscitation is critically important.
6) ING. OCTREOTIDE
mechanism:
Like somatostatin, octreotide also decreases the release of growth stimulating hormones, decreases blood flow to the digestive organs, and inhibits the release of digestive hormones such as serotonin, gastrin, vasoactive intestinal peptide, secretin, motilin, and pancreatic polypeptide.
Octreotide is useful in overdose management of sulfonylurea type hypoglycemic medications, when recurrent or refractory to parenteral dextrose. Mechanism of action is the suppression of insulin secretion.
7) ING. PANTOP
mechanism:The mechanism of action of pantoprazole is to inhibit the final step in gastric acid production. In the gastric parietal cell of the stomach, pantoprazole covalently binds to the H+/K+ ATP pump to inhibit gastric acid and basal acid secretion. The covalent binding prevents acid secretion for up to 24 hours and longer.
8) ING. THIAMINE
mechanism:Vitamin B1 (thiamin) is indispensable for normal function/health of pancreatic cells due to its critical role in oxidative energy metabolism, ATP production, and in maintaining normal cellular redox state.
9) ING. TRAMADOL
mechanism:Tramadol is a centrally acting analgesic with a multimode of action. It acts on serotonergic and noradrenergic nociception, while its metabolite O-desmethyltramadol acts on the µ-opioid receptor. Its analgesic potency is claimed to be about one tenth .
2) GASTROENTEROLOGY CASE 2
CASE OF 25 YEAR OLD MAN ,WITH SEVERE EPIGASTRIC PAIN
Link to patient details:
What is causing the patient's dyspnea? How is it related to pancreatitis?
Ans :the cause of dyspnea might be PLEURAL EFFUSION
2) Name possible reasons why the patient has developed a state of hyperglycemia.
Ans:
*This hyperglycemia could thus be the result of a hyperglucagonemia secondary to stress
* the result of decreased synthesis and release of insulin secondary to the damage of pancreatic β-cells
* elevated levels of catecholamines and cortisol
3)What is the reason for his elevated LFTs? Is there a specific marker for Alcoholic Fatty Liver disease?
Ans:
LFT are increased due to hepatocyte injury
*If the liver is damaged or not functioning properly, ALT can be released into the blood. This causes ALT levels to increase. A higher than normal result on this test can be a sign of liver damage.
*elevated alanine transaminase (ALT) and aspartate transaminase (AST), usually one to four times the upper limits of normal in alcoholic fatty liver.
The reasons for a classical 2:1 excess of serum AST activity compared to serum ALT activity in alcoholic hepatitis have been attributed to
(i) decreased ALT activity most likely due to B6 depletion in the livers of alcoholics
(ii) mitochondrial damage leading to increased release of mAST in serum.
4) What is the line of treatment in this patient?
Plan of action and Treatment:
Ans:nvestigations:
✓ 24 hour urinary protein
✓ Fasting and Post prandial Blood glucose
✓ HbA1c
✓ USG guided pleural tapping
Treatment:
• IVF: 125 mL/hr
• Inj PAN 40mg i.v OD
• Inj ZOFER 4mg i.v sos
• Inj Tramadol 1 amp in 100 mL NS, i.v sos
• Tab Dolo 650mg sos
• GRBS charting 6th hourly
• BP charting 8th hourly
3) GASTROENTEROLOGY CASE 3
A 45 year old Female patient with Fever, Pain abdomen, Decreased Urine output and Abdominal distension
Link to patient details:
1)what is the most probable diagnosis in this patient?
1) What is the most probable diagnosis in this patient?
Ans:Differential Diagnosis:
· Ruptured Liver Abscess.
· Organized collection secondary to Hollow viscous Perforation.
· Organized Intraperitoneal Hematoma.
· Free fluid with internal echoes in Bilateral in the Subdiaphragmatic space.
· Grade 3 RPD of right Kidney
The most probably diagnosis is there is abdominal hemorrhage. This will give reasoning to the abdominal distention, and the blood which is aspirated.
2) What was the cause of her death?
Ans:After leaving the hospital, the patient went to Hyderabad and underwent an emergency laparotomy surgery. The patient passed away the next day. Cause of her death can be due to complications of laparotomy surgery such as, hemorrhage (bleeding), infection, or damage to internal organs.
3) Does her NSAID abuse have something to do with her condition? How?
Ans: NSAID-induced renal dysfunction has a wide spectrum of negative effects, including decreased glomerular perfusion, decreased glomerular filtration rate, and acute renal failure. Chronic NSAIDs use has also been related to hepatotoxicity. While the major adverse effects of NSAIDs such as gastrointestinal mucosa injury are well known, NSAIDs have also been associated with hepatic side effects ranging from asymptomatic elevations in serum aminotransferase levels and hepatitis with jaundice to fulminant liver failure and death.
NEPHROLOGY AND UROLOGY
1) NEPHROLOGY CASE 1
A52 year old male patient with burning micturition, shortness of breath and fever
Link to patient details:
1)What could be the reason for his SOB ?
Ans- His sob was is due to Acidosis which was caused by Diuretics
2. Reason for Intermittent Episodes of drowsiness
Ans-Hyponatremia was the cause for his drowsiness
3.why did he complaint of fleshy mass like passage inurine?
Ans-plenty of pus cells in his urine passage appeared as
fleshy mass like passage to him
4. What are the complicat ions of TURP that he may have had
Ans-
Difficulty micturition
Electrolyte imbalances
Infections
2) NEPHROLOGY CASE 2
An 8 year old with frequent urination
Link to patient details:
1)why is the child excessively hyperactive without much social etiquette?
Ans: From the history of excessive hyperactivity, impulsiveness, lacking attentivity,a thought goes towards attention deficit hyperactivity and in association urination disorders.
2)Why doesn't the child have excessive urination at night time?
Ans: since the child does not get the urge to urinate when he is asleep, there can be a chance of manifestation being psychosomatic, or as a result of an undiagnosed anxiety disorder.
3)How would you want to manage the patient to relieve him of his symptoms?
Ans: daytime overactive bladder is a common pediatric problem that usually resolves over time which usually resolves over time with reassurance and relaxation and behavioral therapy.
INFECTIOUS DISEASES (HIV,MYCOBACTERIUM,GASTROENTEROLOGY, PULMONOLOGY)
1)INFECTIOUS DISEASES CASE 1.
A 40 year old lady with dysphagia, fever and cough
Link to patient details:
1.Which clinical history and physical findings are characteristic of tracheo esophageal fistula?
Ans: clinical history and physical finding in this payient that suggest tracheoesophageal fistula is that
-Cough occurs on taking food and liquids
(which was initially non productive then associated with sputum which is white in color , moderate in quantity and non foul smelling)
2)What are the chances of this patient developing immune reconstitution inflammatory syndrome? Can we prevent it?
Ans : Immune reconstitution inflammatory syndrome (IRIS) occurs in two forms:
"unmasking" IRIS refers to the flare-up of an underlying, previously undiagnosed infection soon after antiretroviral therapy (ART) is started;
"paradoxical" IRIS refers to the worsening of a previously treated infection after ART is started.
*Patients with mycobacterial disease at the time of initiation of ART are at higher risk of developing IRIS with an approximate risk of 15%. Patients originating from endemic areas for tuberculosis and cryptococcal disease are at higher risk of developing IRIS.
B)How can immune reconstitution inflammatory syndrome be prevented?
*The most effective prevention of IRIS would involve initiation of ART before the development of advanced immunosuppression. IRIS is uncommon in individuals who initiate antiretroviral treatment with a CD4+ T-cell count greater than 100 cells/uL.
*Aggressive efforts should be made to detect asymptomatic mycobacterial or cryptococcal disease prior to the initiation of ART, especially in areas endemic for these pathogens and with CD4 T-cell counts less than 100 cells/uL.
*Two prospective randomized studies are evaluating prednisone and meloxicam for the prevention of paradoxical TB IRIS.
INFECTIOUS DISEASES AND HEPATOLOGY
HEPATOLOGY CASE 1
A 55 year old male patient with abdominal pain, decreased appetite, fever.
Link to patient details:
1)Do you think drinking locally made alcohol caused liver abscess in this patient due to predisposing factors
present in it ?
What could be the cause in this patient?
ans- yes, it could be due to intake of contaminated toddy
2Q)what is the etiopathogenesis of liver abscess in a chronic alcoholic patient?(since 30 yrs - 1 bottle/day)
Ans - according to some studies, alcoholism mainly consuming locally prepared alcohol plays a major role as a predisposing factor for the formation of liver abscesses that is both amoebic as well as pyogenic liver abscess because of the adverse effects of alcohol over the Liver. It is also proven that Alcoholism is never an etiological factor for the formation of liver abscess.
3Q)is liver abscess is more common in right lobe?
Ans-yes right lobe is involved due to its moreblood supply
4Q) what r the indications for usg guided aspiration of liver abscess
Ans- Indications for USG guided aspiration of liver abscess
1. Large abscess more than 6cms
2. Left lobe abscess
3.Caudate lobe abscess
4. Abscess which is not responding to drugs
HEPATOLOGY CASE 2
A 21 year old male student with abdominal pain and fever
Link to patient details:
1)Cause of liver abcess in this patient ?
Ans:cause of liver abcess in this patient is ENTAMOEBA HISTOLYTICA
2) How do you approach this patient ?
Ans:APPROACH IN THE PATIENT OF AMOEBIC LIVER ABCESS
3) why do we treat here ; both amoebic and pyogenic liver abcess?
Ans:we treat the paient for both amoebic and pyogenic abcess so that we dont rely only on anti-amebic therapy and insure comple treatment of the cause
4) Is there a way to confirmthe definitive diagnosis in this patient?Ans:he confirmatory test for amoebic abcess is
*Serologic testing is the most widely used method of diagnosis for amebic liver abscess. In general, the test result should be positive, even in cases when the result of the stool test is negative (only extraintestinal disease).
*The diagnosis of amebic liver abscess was based on four or more of the following criteria:
(i) a space-occupying lesion in the liver diagnosed by ultrasonography and suggestive of abscess,
(ii) clinical symptoms (fever, pain in the right hypochondrium (often referred to the epigastrium), lower chest, back, or tip of the right shoulder),
(iii) enlarged and/or tender liver, usually without jaundice,
(iv) raised right dome of the diaphragm on chest radiograph, and
(v) improvement after treatment with antiamebic drugs (eg: Metronidazole)
INFECTIOUS DISEASES (MUCORMYCOSIS,OPHTHALMOLOGY, OTORHINOLARYNGOLOGY, NEUROLOGY)
CASE 1
A 50-year-old male with altered sensorium
Link to patient details:
1) What is the evolution of the symptomatology in this patient in terms of an event timeline and where is the anatomical localization for the problem and what is the primary etiology of the patient's problem?
Ans : Evolution of symptomatology
Fever since 10 days
Facial puffiness and periorbital edema for 4 days
Weakness of right upper limb and lower limb since 4 days
Altered sensorium since 2 days
Patient was apparently asymptomatic 3 years back and went to local hospital in/v/o Regular checkup and came to diagnosed with Hypertension .
And on 18/04/21 He went to local PHC for COVID 19 vaccination.. Since that night patient is complaining of Fever associated with chills and rigors, high grade fever, no diurnal variation which was relieved on medication...
Followed by patient is having similar complaints after three days
On 28/04/21 , c/o Generalized weakness and facial puffiness and periorbital edema.. And also patient is in drowsy state..
On 04/05/21, patient presented to casualty In altered state with facial puffiness and periorbital edema and weakness of right upper limb and lower limb...
*the anatomical location of the problem is MAXILLARY SINUS
(primary disease is initiated in the upper or lower airways and is associated with the clinical development of sinusitis, rhinocerebral mucormycosis, )*primary etiology of the patients' problem is IMMUNOSUPPRESSION CAUSED BY DIABETES MELLITUS.
2) What is the efficacy of drugs used along with other non pharmacological treatment modalities and how would you approach this patient as a treating physician?
Ans: Inj Liposomal amphotericin B according to creatinine clearance
Loading dose 30mg/IV over 2-6 hrs
Maintenance dose 60mg / IV once a day
He has been given 200mg of itraconazole (the only drug currently available) adjusted to his creatinine clearance which is 43ml/min
Deoxycholate ampB requirement is 70mg per day
Affordability issues:
The cost of 50mg is 500to 700rupees
Liposomal ampB requirement is 350mg once daily
Where 50mg costs 2400 to 3000 rupees per day
Even the busiest pharmacy in Hyderabad (we called Osmania Medical College pharmacy) doesn't have deoxycholate.
Liposomal is still available for 30% lesser price. Posaconazole price is 15k starting.
And he was referred to Osmania general hospital where he was given one dose of deoxycholate amphotericin B and patient has died On 6th may around 10 am.
3) What are the postulated reasons for a sudden apparent rise in the incidence of mucormycosis in India at this point of time?
Earlier, mucormycosis was commonly spotted in people suffering from diabetes mellitus, a condition where one's blood sugar (glucose) levels are abnormally high. Cancer patients undergoing chemotherapy, those who have had a transplant, and people taking immunosuppressants (medications that weaken the immune system) also used to get it. But now due to Covid-19 and its treatment, an increase in the number of cases is being witnessed
Medicines used in treating Covid-19 tend to bring down the count of lymphocytes. Lymphocytes are one of the three types of white blood cells whose job is to defend our body against disease-causing pathogens such as bacteria, viruses, and parasites. The reduced count of lymphocytes leads to a medical condition called lymphopenia, making way for opportunistic fungal infection in Covid-19 patients.
There is a higher chance of occurrence of mucormycosis in patients whose immune system is not functioning well, and since Covid-19 treatment tends to suppress the working of the immune system, it places such patients at a higher risk of contracting the black
INFECTIOUS DISEASES
Below is the link to view my master sheet on covid 19 cases
https://docs.google.com/spreadsheets/d/1_jsUNEJcKftN0EqPutBXsRLyZSkdjDk9S72oBe41z6Y/edit?usp=sharing
COVID 19 WITH COMORBIDITY ( PULMONOLOGY, RHEUMATOLOGY)
CASE 1
A 58-YEAR-old female with fever and shortness of breath
https://nikhilasampathkumar.blogspot.com/2021/05/covid-pneumonia-in-pre-existing-case-of.html
1) How does the pre-existing ILD determine the prognosis of this patient?
Ans: The prognosis of COVID-19 patients with pre-existing ILD is significantly worse than that of non-ILD patients. And more, aggravated inflammatory responses and coagulation dysfunction appear to be the critical mechanisms in the COVID-19 patients with ILD.
Patients with preexisting interstitial lung disease (ILD) may be at high risk for severe coronavirus disease (COVID-19) because of impaired lung function, propensity to develop acute exacerbation of pulmonary fibrosis or immunomodulatory medications that may interact with viral clearance or pathogenesis. Previous studies found that patients with ILDs had an increased risk of death compared with control subjects matched for age, sex, comorbidities, and/or race.
2). Given the history of autoimmune disease in the patient, how does the administration of steroids for COVID affect her RA and hypothyroidism?
Ans: The administration of steroids in this patient affects her rheumatoid arthritis. Dexamethasone is used in the treatment of arthritis or autoimmune conditions like rheumatoid arthritis, lupus, and gout.
Research into using this drug to treat coronavirus was conducted as part of the RECOVERY (Randomised Evaluation of COVID-19 Therapy) trial by the University of Oxford to test a range of potential treatments for COVID-19.
Due to the immune-suppressing properties of dexamethasone, researchers decided to test its effectiveness in treating coronavirus patients with severe respiratory symptoms.
Researchers found that dexamethasone reduced deaths by one-third in ventilated patients, and by one fifth in other patients receiving oxygen only. There was no benefit among those patients who did not require respiratory support.
Dexamethasone is a readily accessible drug, and the first that’s shown to improve survival rates in COVID-19.
While it is effective for treating coronavirus patients requiring respiratory support for severe respiratory symptoms, guidelines should still be followed for people taking the drug to treat inflammatory or autoimmune conditions.
HYDROXYCHLOROQUINE’S SIDE EFFECTS IN COVID-19 PATIENTS
Adverse outcomes from the drug tend to result from taking it in large doses or for a long period of time, or from hydroxychloroquine’s interactions with other medications. This helps explain why some patients with COVID-19 have developed heart arrhythmias (unusual heart rhythms) and other issues in response to the drug.
Some patients were given large doses — much larger than what is prescribed for patients with lupus and other conditions. And COVID-19 patients are often in very poor health by the time they’re treated, with heart complications and other issues that people with autoimmune disease generally don’t have.
3.Would this patient have an increased risk for post covid autoimmune response compared to patients without a history of autoimmune disease?
Ans: Yes, the patient may have increased risk for post Covid autoimmune response With the progression of the COVID-19 pandemic, there have been different reports about the development of autoimmune diseases once the infection is controlled. After entering the respiratory epithelial cells, SARS-CoV-2—the virus that causes the disease—triggers a severe inflammatory state in some patients known as “cytokine storm” and the development of thrombotic phenomena—both conditions being associated with high mortality. Patients additionally present severe lymphopenia and, in some cases, complement consumption and autoantibody development. There is a normalization of lymphocytes once the infection is controlled. After this, autoimmune conditions of unknown etiology may occur.A hypothesis for the development of post-COVID-19 autoimmunity is proposed based on the consequences of both a transient immunosuppression (both of innate and acquired immunity) in which self-tolerance is lost and an inappropriate form of immune reconstitution that amplifies the process.
Conclusion: The development of autoimmune conditions subsequent to COVID-19 infection could be related to both factors: transient immunosuppression of innate and acquired immunity leading to a loss of self-tolerance to self-antigens, and a form of inappropriate immune reconstitution in individuals with predisposing conditions of autoimmunity.
4.Why was she prescribed clexane (enoxaparin)?
Ans: clexane (enoxaparin) is prescribed because of below reasons .In a specific section, the interim guidance recently released (WHO, 2020) recommends thromboprophylaxis with either unfractionated or low molecular weight heparin (LMWH), since, as discussed earlier in this review, acute infections are strong prothrombotic stimuli and these patients are at increased risk of venous thromboembolism (VTE).
Severe and critically ill COVID patients with prolonged immobilization are inherently at high risk of VTE, and pulmonary embolism (PE) should also be considered in those with clinical deterioration with hypoxia and hemodynamic instability.
COVID 19 CASE 2
COVID CASE WITH DIABETES
A 50-year-old female with viral pneumonia secondary to covid 19
Link to the patient case report log:
1) Since patient didn't show any previous characteristic diabetes signs, did the Covid-19 infection aggravate any underlying condition and cause the indolent diabetes to express itself? If so what could be the biochemical pathways that make it plausible?
Ans: COVID-19 infection can cause a lot of serious, sometimes lingering health problems, like lung damage, kidney damage and ongoing heart issues. Lately, research has suggested it may also cause the sudden onset of insulin-dependent diabetes.
Biochemical pathways:
Beta cells in the pancreas contain a significant number of so-called ACE2 receptors. These receptors are believed to be where the spike protein from the coronavirus attaches to cells. Beta cells produce insulin, a hormone that helps usher the sugar from foods into the body's cells for fuel. The authors theorized that a coronavirus infection, which affects the ACE2 receptors, might also damage beta cells in the pancreas.
This process is similar to what's believed to occur in type 1 diabetes. The immune system mistakenly turns on healthy cells (autoimmune attack) after a viral infection and damages or destroys beta cells, possibly causing type 1 diabetes.
2) Did the patient's diabetic condition influence the progression of her pneumonia?
Ans: Diabetic subjects may have increased susceptibility to pneumonia for several reasons. They are at increased risk of aspiration, hyperglycemia, decreased immunity, impaired lung function, pulmonary microangiopathy, and coexisting morbidity.
3.What is the role of D Dimer in the monitoring of covid? Does it change management or would be considered overtesting?
Ans: D-dimer is commonly elevated in patients with COVID-19. D-dimer levels correlate with disease severity and are a reliable prognostic marker for in-hospital mortality in patients admitted for COVID-19.
Clexane (enoxaparin) can be given .
COVID 19 CASE 3
COVID 19 SEVERE
A 26-year-old female with fever and shortness of breath
Link to the complete case report log:
1. Why was this patient given noradrenaline?
Ans: As the patient is diagnosed by AKI,to restore arterial pressure with the aim of sustaining organ perfusion pressure, the administration of systemic vasopressor agents, such as noradrenaline, becomes necessary. Norepinephrine infusions can decrease splanchnic and renal blood flow under normal circulatory conditions, as well as during essential hypertension and hypovolemic hypotension.
2.What is the reason behind testing for LDH levels in this patient?
Ans: LDH is a favorable prognostic biomarker with high accuracy for predicting in-hospital mortality in severe and critically ill patients with COVID-19. This may direct physicians worldwide to effectively prioritize resources for patients at high risk of death and to implement more aggressive treatments at an earlier phase to save patients' lives.
Lactate dehydrogenase (LDH) is a cytoplasmic enzyme that is widely expressed in tissues. The enzyme converts pyruvate, which is the final product of glycolysis, to lactate when oxygen is in short supply. LDH comprises two separately enclosed subunits, resulting in five isozymes. Each isozyme is expressed in a specific organ: LDH 1 in cardiomyocytes, LDH 3 in lung tissue, and LDH 5 in hepatocytes. Increased LDH was observed in different conditions such as tissue injury, necrosis, hypoxia, hemolysis, or malignancies. Additionally, Tao et al. found that LDH was associated with death in patients with community-acquired pneumonia (CAP) caused by viruses.
A growing number of studies demonstrated that elevated LDH value was associated with significantly increased mortality in patients with COVID-19.
3.What is the reason for switching from BiPAP to mechanical ventilation with intubation in this patient? What advantages did it provide?
Ans: As the patient SpO2 was below 30%, they switched from BiPaP to mechanical ventilation with intubation.
A ventilator might be considered if your breathing problems are more severe. A ventilator is used to breathe for you when you can't breathe on your own.
Mechanical ventilation might be considered if you have:
• New or long-term severe lung problems
• Brain damage
• An injury to your spinal cord
• Severe weakness of the muscles in your chest
Advantages:
They might make it easier to breathe.
They might help breathe while recovering from a serious illness.
They might prolong life, depending on the condition. People with some conditions live for years using mechanical ventilation.
COVID 19 CASE 4 -MILD
A 29-year-old male patient with viral pneumonia secondary to covid 19
Link to the case report log:
1. Is the elevated ESR due to covid related inflammation?
ans: Erythrocyte sedimentation rate (ESR) is a blood test. It measures how quickly erythrocytes, or red blood cells, separate from a blood sample that has been treated so the blood will not clot.
The sustained high level of ESR possibly brings a negative effect on COVID-19 patients' prognosis
However, the elevation in esr cannot be explained based on the present knowledge of Covid
2. What was the reason for this patient's admission with mild covid? What are the challenges in home isolation and the harms of hospitalization?
ans: after 14 days of isolation he got tested again for COVID-19 which was positive. He then developed fever since 4 days, cough which was productive since 4 days, and shortness of breath grade 3 since 2 days. He also had fatigue. He lost the sense of taste and smell.
Since the patient has an SOB of grade 3. This poses a challenge for home isolation.
Patients with COVID-19 had almost 19 times the risk for acute respiratory distress syndrome (ARDS) than did patients with influenza, (adjusted risk ratio [aRR] = 18.60; 95% confidence interval [CI] = 12.40–28.00), and more than twice the risk for myocarditis (2.56; 1.17–5.59), deep vein thrombosis (2.81; 2.04–3.87), pulmonary embolism (2.10; 1.53–2.89), intracranial hemorrhage (2.85; 1.35–6.03), acute hepatitis/liver failure (3.13; 1.92–5.10), bacteremia (2.46; 1.91–3.18), and pressure ulcers (2.65; 2.14–3.27). The risks for exacerbations of asthma (0.27; 0.16–0.44) and chronic obstructive pulmonary disease (COPD) (0.37; 0.32–0.42) were lower among patients with COVID-19 than among those with influenza. The percentage of COVID-19 patients who died while hospitalized (21.0%) was more than five times that of influenza patients (3.8%), and the duration of hospitalization was almost three times longer for COVID-19 patients.
COVID 19 CASE 5
COVID 19 AND COMORBIDITY ( ALTERED SENSORIUM, AZOTEMIA, HYPOKALEMA)
A 45 year old male with covid 19 and comorbidities
Link to the case report log:
1) What was the reason for coma in this patient?
ans:The patient has an spo2 of 20%. This might have lead to cerebral hypoxia thus leading to coma.
Also, low blood potassium can make you short of breath, as it can cause the heart to beat abnormally. This means less blood is pumped from your heart to the rest of your body
Thus low spo2 and thus coma
2) What were the competency gaps in hospital 1 Team to manage this intubated comatose patient that he had to be sent to hospital 2? Why and how did hospital 2 make a diagnosis of hypokalemic periodic paralysis? Was the coma related?
ans:Hospital 1 might not have correlated Severe weakness of 4 limbs with low values of potassium which hospital 2 has diagnosed.
Yes, coma is related to Hypokalemia periodic paralysis as it might have caused cerebral hypoxia.
3) How may covid 19 cause coma?
ans:After cessation of sedatives, the described cases all showed a prolonged comatose state. unconsciousness after prolonged periods of mechanical ventilation in the ICU.
COVID 19 CASE 6-SEVERE
A 65 year old male with severe viral pneumonia secondary to covid 19
Link to the case report log:
12
1. What was the cause of his altered sensorium?
ans:Can be any of the following reasons
An altered state is any mental state(s), induced by various physiological( increased hospital stay) , psychological( mental depression due to isolation), or pharmacological maneuvers or agents( drugs of COVID)
2. What was the cause of death in this patient?
ans:This patient is an elderly chronic alcoholic and smoker.
This might have delayed his healing process thus causing death Also he had elevation LFT and RFT values
COVID 19 CASE 8-MODERATE
35YR/M WITH VIRAL PNEUMONIA SECONDARY TO COVID 19 INFECTION
Link to the complete case report log
1. Can psoriasis be a risk factor for severe form of COVID?
Ans: Elderly psoriasis patients and/or patients using conventional immunosuppressive regimens and biologic agents are at higher risk for infectious diseases.
But the frequency of COVID-19 does not increase in patients using immunosuppressants, including those receiving biological therapy with a diagnosis of psoriasis
2. Can the increased use of immunomodulatory therapies cause further complications in the survivors?
Ans:According to the present knowledge on Covid,there is no indication that people taking immunomodulatory drugs for other diagnosed conditions should be concerned that their medication increases their risk for severe COVID-19,"
3. Is mechanical ventilation a risk factor for worsened fibroproliferative response in COVID survivors?
Ans: patients of Covid with greater fibrotic changes required more prolonged mechanical ventilation, and this in turn was associated with an increased severity of systemic organ failure.
Hence Mechanical ventilation is risk factor
COVID-19 CASE -9
COVID-19-DENOVO DIABETES
A 45 YEAR OLD FEMALE WITH VIRAL PNEUMONIA SECONDARY TO COVID 19
Link to Case report log:
1 )What is the type of DM the patient has developed ?(is it the incidental finding of type 2 DM or virus induced type 1DM )?
Ans:SARS-CoV-2 could directly impair insulin production of beta-cells, diminishing its function and disturb glucose metabolism, would that be enough to com- promise insulin production in a long-term manner and induce type 1 diabetes
CoV-2: that develop de novo hyperglycemia with difficult metabolic control, since there is downregulation of the ACE2 receptor which is internalized.
 New onset DM in patient may be responsible for late recovery as the virus may thrive in an environment of elevated blood glucose.
New onset DM in patient may be responsible for late recovery as the virus may thrive in an environment of elevated blood glucose.
2)•Could it be steroid induced Diabetes in this patient?
Ans : yes
In recent years, it has also been proposed that stimulation of the ACE2-Ang(1-7)-Mas axis could be protective against deleterious effects of diabetic nephropathy, hypertension and diabetic retinopathy and that patients with diabetes have lower Angiotensin-(1-7) levels and lower activity of ACE2. These findings are consistent with the clinical features of patients infected by SARS- -CoV-2: that develop de novo hyperglycemia with difficult metabolic control, since there is downregulation of the ACE2 receptor which is internalized.
COVID-19 CASE -10
Comparing the two covid patients
1)What are the known factors driving early recovery in covid?
Ans: patient didn't develop denovo Diabetes
There is no prolonged fever compared to the patient 1
There is no severe inflammatory process on the lungs and there is no cytokine storm in this patient
These causes paved way for her early recovery .
COVID-19 CASE -11
Covid moderate with first time detected diabetes:
Link to Case report log :
1)How is the diabetes related to the prognosis of COVID patients? What are the factors precipitating diabetes in a patient developing both covid as well as Diabetes for the first ?
Ans: The problem people with diabetes face is they’re more likely to have worse complications if they get it, not greater chance of getting the virus. Also, the more health conditions someone has (for example, diabetes plus heart disease), adds to their risk of getting those serious complications from COVID-19. Older people are also at higher risk of complications if they get the virus.
2. Why couldn't the treating team start her on oral hypoglycemics earlier?
Ans: Because she was diagnosed with Diabetes after admitting in hospital. So the doctors started her on hypoglycemic drugs as her GRBS levels are high.
COVID-19 CASE 12
COVID-19 MODERATE TO SEVERE
Moderate to severe covid with prolonged hospital stay:
1) What are the potential bioclinical markers in this patient that may have predicted the prolonged course of her illness?
The potential biochemical markers in this patient are
Elevated levels of
LFT- Total bilirubin : 1.24 mg/dl
Direct bilirubin : 0.67 mg/dl
SGOT : 73 units/ lit
sGPT : 80 units/ lit
ALP : 342 units/ lit
RFT Blood urea : 34 mg/dl
Sodium : 150 meq/lit
Potassium : 5.2 meq/lit
SERUM LDH 571 units/lit
FBS 332 mg /dl
COVID-19 CASE -13
Severe covid with first diabetes
Link to Case report log :
1. What are the consequences of uncontrolled hyperglycemia in covid patients?
Ans: Adults with diabetes or uncontrolled hyperglycemia hospitalized with COVID-19 experienced a longer length of stay and markedly higher mortality compared with adults without diabetes or uncontrolled hyperglycemia, according to findings published in the Journal of Diabetes Science and Technology.
2.Does the significant rise in LDH suggests multiple organ failure?
Ans: Yes the significant rise in LDH levels can lead to multiple organ failure due to tissue injury.
Lactate dehydrogenase (LDH) is an enzyme required during the process of turning sugar into energy for your cells. LDH is present in many kinds of organs and tissues throughout the body, including the liver, heart, pancreas, kidneys, skeletal muscles, lymph tissue, and blood cells.
When illness or injury damages your cells, LDH may be released into the bloodstream, causing the level of LDH in your blood to rise. High levels of LDH in the blood point to acute or chronic cell damage, but additional tests are necessary to discover its cause. Abnormally low LDH levels only rarely occur and usually aren’t considered harmful.
Because LDH is present in so many types of cells, high levels of LDH may indicate a number of conditions. Elevated levels of LDH can include:
blood flow deficiency
cerebrovascular accident, also known as a stroke
certain cancers
heart attack
hemolytic anemia
infectious mononucleosis
liver disease, such as hepatitis
muscle injury
muscular dystrophy
pancreatitis
tissue death
use of alcohol or certain drugs
sepsis and septic shock
COVID-19 CASE-14
Long covid with sleep deprivation and ICU psychosis
Link to Case report log:
1)Which subtype of ICU psychosis did the patient land into according to his symptoms?
Ans : Delirium may be cause of ICU psychosis in this patient.
2)What are the risk factors in the patient that has driven this case more towards ICU pyschosis?
Ans: Risk factors for developing the icu psychosis were:
1)shortness of breath which is 10-15 days of duration, Insideous in onset, gradually progressive and was of Grade 3 (NYHA) with no known aggravating factors and was relieved on oxygen supplementation.
2)He had a Cerebrovascular Accident (CVA) 2 years ago
3)Occasional alcohol intake (monthly once)
3)The patient is sleep deprived during his hospital stay..Which do u think might be the most propable condition?
Ans : ICU psychosis causing sleep deprivation
Because patient had Delirium and most of the patient's with Delirium are hyperactive and patient feels irritable, full of energy and probably this causes the patient depriving from sleep.
4)What are the drivers toward current persistent hypoxia and long covid in this patient?
Ans:Many patients present with a remarkable disconnect in rest between profound hypoxemia yet without proportional signs of respiratory distress (i.e. happy hypoxemia) and rapid deterioration can occur. This particular clinical presentation in COVID-19 patients contrasts with the experience of physicians usually treating critically ill patients in respiratory failure and ensuring timely referral to the intensive care unit can, therefore, be challenging.
COVID-19 CASE -15
Moderate Covid with comorbidity (Trunkal obesity and recent hyperglycemia)
Link to Case report Log:
1. As the patient is a non- diabetic, can the use of steroids cause transient rise in blood glucose?
Ans:Yes, Increase in the blood glucose might be due to the use of steroids, in this case Dexamethasone
2. If yes, can this transient rise lead to long term complication of New-onset diabetes mellitus?
Ans: High blood glucose levels whilst taking steroids may subside after one stop taking steroids, however, some people may develop type 2 diabetes which will need to be managed for life.
Type 2 diabetes is more likely to develop following longer term usage of steroids, such as usage of oral corticosteroids for longer than 3 months.
3. How can this adversely affect the prognosis of the patient?
Ans:The reason for worse prognosis in people with diabetes is likely to be multifactorial, thus reflecting the syndromic nature of diabetes. Age, sex, ethnicity, comorbidities such as hypertension and cardiovascular disease, obesity, and a pro-inflammatory and pro-coagulative state all probably contribute to the risk of worse outcomes
4. How can this transient hyperglycemia be treated to avoid complications and bad prognosis?
Ans: At admission: pre-meal BG: 150 to 180 mg/dl and/or post-meal BG 200 to 250 mg/dl)
If there is an anticipated delay in consulting endocrinologist/physician, initiate on Tab Metformin (either immediate or sustained release) 500 mg BD and a Gliptin (Tab Vildagliptin 50 mg BD or Tab Sitagliptin 100 mg OD or Tab Linagliptin 5 mg OD or Tab Teneligliptin 20 mg OD)
Indication: At admission: pre-meal BG: ≥180 mg/dl or post-meal BG ≥250 mg/dl
A. Total daily dose (TDD) = 0.4 units/kg/day (age > 65 yr, nephropathy or liver disease, use 0.2 units/kg/day)
B. Total daily dose is divided equally into 4 doses (25% each): 3 doses are for bolus insulin (Regular insulin 30 min before breakfast, before lunch and before dinner) and 1 dose for basal insulin (Inj. NPH insulin at bed time/ 2 hours after dinner)
If pre-meal BG value is 140 to 180 mg/dl and/or post-meal BG value is 180 to 250 mg/dl → consult endocrinologist/physician for OAD optimization
B. If pre-meal BG value ≥180 mg/dl and/or post-meal BG value ≥250 mg/dl despite being on OAD → start basal-bolus insulin regimen using calculation mentioned in section 3A (Kindly note that in this particular scenario, OADs apart from Metformin and Gliptins need to be stopped).
5. What is thrombophlebitis fever?
Ans:Thrombophlebitis is when a blood clot Any veins and slows the blood flow in the vein. It may be due prolonged use of IV cannula.
This causes fever
6. Should the infusion be stopped inorder to control the infusion thrombophlebitis? What are the alternatives?
Ans: There is no need to stop infusion to control Theombophlebitis. Instead change the IV cannula to opposite or another site. If there is pain at that site use aspirin or ibuprofen
COVID-19 CASE-16
Mild to moderate covid with hyperglycemia
1. What could be the possible factors implicated in elevated glycated HB ( HBA1c ) levels in a previously Non-Diabetic covid patient?
Ans: the patients was heterozygous for Hb-SF that leads to falsely elevated HbA1c levels. When evaluated by affinity column HPLC, her HbA1c levels were in the normoglycemic range
The Hb-SF variant substitutes a neutral amino acid for a charged one (valine for methionine), which decreases the transit time in the ion exchange column; this causes it to co-elute together with HbA1c and produce a falsely elevated value.
While this is only the fourth reported case of Hb-SF, this case study emphasizes the importance of the many Hb variants that could interfere with routine laboratory tests. The authors conclude that clinicians should consider multiple factors besides HbA1c in diabetes assessment and diagnosis, and that abnormal Hb variants could be driving increased HbA1c levels in patients who do not have symptoms consistent with diabetes and normal blood glucose levels.
2) What is the frequency of this phenomenon of New Onset Diabetes in Covid Patients and is it classical type 1 or type 2 or a new type?
Ans: over 14 percent of people with severe COVID-19, who were analyzed during the research developed diabetes (both type 1 and type 2 diabetes). Notably, some of them had no pre-existing risk factors for the disease.
COVID-19 causing virus affects your pancreas, attacks its beta cells, and disrupts insulin secretion in the body. According to a few doctors, medicines prescribed to severely affected COVID-19 patients sometimes lead to an increase in blood sugar level and that may be a reason behind the onset of diabetes in them.
3)How is the prognosis in such patients?
Ans: Diabetes causes an increase in risk of thromboembolic events as it is tied to a prothrombotic state that results from an imbalance of clotting factors and fibrinolysis. COVID-19 increases coagulation activity even further. The endothelial dysfunction linked to hypoxia can cause intravessel coagulation during an infection. Anticoagulation therapy in patients with COVID-19 seems to improve prognosis.
4)Do the alterations in glucose metabolism that occur with a sudden onset in severe Covid-19 persist or remit when the infection resolves?
Ans: Covid-19 on people with diabetes, in the subsequent three months following a positive Covid-19 report, blood glucose levels were found to have increased by almost 28 percent in the first month, 17 percent in the second month and 11 percent in the third month.
5)Why didn't we start him on Oral hypoglycemic agents earlier?
Ans: FDA-approved indications for the use of oral hypoglycemic drugs primarily focus on type 2 diabetes mellitus.
May be the patient might developed diabetes type 1.
COVID-19 CASE 17
Covid 19 with hypertension comorbidity
1 )Does hypertension have any effect to do with the severity of the covid infection.If it is, Then how?
Ans: Severity of COVID-19 illness is skewed towards the elderly population who have a higher prevalence of hypertension.
SARS-CoV-2 and Interaction with the Renin-Angiotensin Aldosterone System
ACE2 is a modulator of the RAAS, a critical neurohormonal pathway that regulates blood pressure and fluid balance.12 The end product of the RAAS, angiotensin II, is a key vasoactive hormone that binds to angiotensin II receptor type 1 (AT1) located in the heart, lungs, blood vessels, kidneys, and adrenal glands, and it plays a central role in myocardial hypertrophy and fibrosis, inflammation, vascular remodeling, and atherosclerosis.13 ACE2 is expressed in many human tissues including the nasal epithelium, heart, kidneys, and lungs, and inactivates angiotensin II diminishing its vasoconstrictive and myoproliferative effects.14
SARS-CoV-2 binds to the ACE2 receptor via its spike (S) protein to allow entry into host cells. This complex is endocytosed leading to down-regulation of ACE2 and resulting in local accumulation of angiotensin II. Severe respiratory illness is a hallmark of COVID-19 and a primary cause of morbidity- and mortality-local activation of the RAAS is proposed as a mechanism for severe lung injury.
2.what is the cause for pleural effusion to occur?
Ans: Pleural effusion is an uncommon finding in coronavirus infection.
Until this time, there is no clear evidence of how the virus can cause pleural effusion, but it carry an adverse prognostic sign that may indicate a bacterial super-infection in COVID-19 pneumonia.
About 20% of pleural effusions are of unknown aetiology despite fluid analysis, hence the requirement for more invasive diagnostic procedures like pleural biopsy under thoracoscopy guide.The prevalence of pleural effusion is 5–10%
Pleural effusion may present as a complication in patients with coronavirus disease; however, there is still scanty of data to support such a claim. More cases to be identified and studied to prove or refute this theory.
COVID-19 CASE 18
Covid 19 with mild hypoalbuminemia
1)What is the reason for hypoalbuminemia in the patient?
Ans:It may be due to pulmonary capillary leakage in lungs , in response to epithelial endothelial damage due to covid infection.
https://pubmed.ncbi.nlm.nih.gov/33411411/2.
2)What could be the reason for exanthem on arms? Could it be due to covid-19 infection ?
Answer:Yes, what the patient is experiencing isknown as viral exanthem which is one of the cutaneous manifestation of COVID-19.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7549735/
3:What is the reason for Cardiomegaly?
Answer:The most probable cause of that appearance is AP view of the chest. When an anteroposterior view is taken, most times the CXR shows false cardiomegaly. To confirm the cardiomegaly a PA view of chest must be taken.
Another possible cause can be Direct Myocardial Cell Injury. The interaction of SARS-CoV-2 with ACE2 can cause changes to the ACE2 pathways, leading to acute injury of the lung, heart, and endothelial cells. A small number of case reports have indicated that SARS-CoV2 might directly infect the myocardium, causing viral myocarditis. However, in most cases, myocardial damage appeared to be caused by increased cardiometabolic demand associated with the systemic infection and ongoing hypoxia caused by severe pneumonia or ARDS
https://www.ncbi.nlm.nih.gov/books/NBK556152/
4:What other differential diagnoses could be drawn if the patient tested negative for covid infection?
Answer:
Possible alternative diagnoses may include:
• Influenza
• Mycoplasma pneumonia
• Parainfluenza
• Respiratory syncytial virus
• Streptococcus pneumonia
• Other viral or bacterial pneumonia.
5:Why is there elevated D-Dimer in covid infection? What other conditions show D-dimer elevation?
Answer:
It is well known that D-dimer are produced during fibrin breakdown and serve as a marker of fibrinolytic activity. A relationship between proinflammatory cytokines and markers of activation of the coagulation cascade, including D-dimer, has been demonstrated in critical patients or patients with sepsis .There is also evidence that under inflammatory conditions, the alveolar haemostatic balance is shifted towards a predominance of prothrombotic activity .In addition, pro-inflammatory cytokines may be involved in endothelial injury, and may activate coagulation and inhibit fibrinolysis in patients with severe sepsis.
D-dimer can be elevated such as in pregnancy, inflammation, malignancy, trauma, liver disease (decreased clearance), heart disease, sepsis or as a result of hemodialysis, CPR or recent surgery)
COVID-19 CASE-20
Covid 19 with first time diabetes
1. Can usage of steroids in diabetic Covid patients increases death rate because of the adverse effects of steroids?
Ans: findings from both observational studies and RCTs confirm a beneficial effect of corticosteroids on short-term mortality and a reduction in need for mechanical ventilation. And although data in the studies were too sparse to draw any firm conclusions, there might be a signal of delayed viral clearance and an increase in secondary infections.
2.Why many COVID patients are dying because of stroke though blood thinners are given prophylactically???
Ans: The results that are in so far suggest that individuals hospitalized, but not severely ill, with COVID-19 who received a full intravenous dose of the common blood thinner heparin were less likely to need vital organ support, including mechanical ventilation, compared to those who received the lower “prophylactic” subcutaneous dose. It’s important to note that these findings are in contrast to results announced last month indicating that routine use of a full dose of blood thinner for patients already critically ill and in the ICU wasn’t beneficial and may even have been harmful in some cases.
2.Does chronic alcoholism have effect on the out come of Covid infection????
If yes,how??
Ans:Though there’s still limited data on the link between alcohol and COVID-19, past evidence shows alcohol consumption can worsen the outcomes from other respiratory illnesses by damaging the lungs and gut, and impairing the cells responsible for immune function.
When someone is exposed to a virus, the body mounts an immune response to attack and kill the foreign pathogen.
In general, the healthier a person’s immune system is, the quicker it can clear out a virus and recover from a disease like COVID-19.
By default, alcohol makes it harder for the immune system to gear up and defend the body against harmful germs.
“Alcohol has diverse adverse effects throughout the body, including on all cells of the immune system, that lead to increased risk of serious infections,”
In the lungs, for example, alcohol damages the immune cells and fine hairs that have the important job of clearing pathogens out of our airway.
If the cells lining a person’s airway are damaged from alcohol, then viral particles, such as COVID-19, more easily gain access, causing immune cells, which fight off infection, to not work as well, leading to increased overall risks of more severe diseases as well as complications,”
COVID-19 CASE -21
Severe Covid with Diabetes
.What can be the causes of early progression and aggressive disease(Covid) among diabetics when compared to non diabetics?
Ans:Diabetes is known to confer increased risk for infections.
patients with COVID-19 with diabetes have a worse prognosis, most probably because of the concurring effect of multiple factors.
The prevalence of diabetes increases with age in both the general population and in patients with COVID-19. Accordingly, the average age of patients with COVID-19 with diabetes is older than those without diabetes.
A separate study6 of a matched population of patients with COVID-19 with and without diabetes reported that survivors were younger than non-survivors, with age 70 years and older being an independent predictor of in-hospital death.
In a retrospective analysis of patients with COVID-19,6 those with diabetes had a greater prevalence of hypertension (56·9%), cardiovascular disease (20·9%), and cerebrovascular disease (7·8%) than those without diabetes (28·8%, 11·1%, and 1·3%, respectively).
2. In a patient with diabetes and steroid use what treatment regimen would improve the chances of recovery?
Ans: Hypoglycemia and hyperglycemia are both predictors for adverse outcomes in hospitalized patients. An optimized glycemic control should be pursued in patients with diabetes and SARS-CoV-2 infection, avoiding hyperglycemic peaks and hypoglycemic events, and blunting inflammatory status in order to reduce the risk of severe complications. The preferred therapeutic options for glucose control with low glucose variability in non-critically ill COVID-19 patients may comprise subcutaneous insulin and GLP-1 receptor agonists (GLP-1RAs).
Insulin associated with a constant glucose monitoring is the first-choice treatment for hyperglycemia in hospital settings. An intensive regimen with basal and prandial insulin analogues is the best treatment for non-critically ill hospitalized patients with good or poor nutritional oral intake, in order to reach the recommended target glucose range of 140–180 mg/dL.
GLP-1RAs are effective glucose-lowering injective drugs used in the treatment of type 2 diabetes.
3.What effect does a history of CVA have on COVID prognosis?
Ans:Yes, stroke has been seen as a manifestation of COVID-19 in various studies showing that 0.9% to 23% COVID-19 patients developed stroke. It has two types of presentations:
Stroke in severely affected COVID-19 patients who initially develop COVID-19 symptoms and later on develop stroke as a multiorgan involvement.
Few studies have shown that some patients present with stroke as an initial manifestation and later on found to have COVID-19, these are young patients without risk factors for brain stroke.
COVID-19 patients have a prothrombotic state which means they have a tendency for the blood to thicken or become sticky which blocks the blood vessels supplying the brain; and the blood supply of a particular part of the brain is cut off resulting in stroke symptoms. It can cause a shower of clots in different parts of the brain or clot can get lodged in one blood vessel and can lead to one territory stroke.
COVID-19 CASE -23
Covid 19 with multiple comorbidities:
http://medicinedepartment.blogspot.com/2021/05/covid-case-report-logs-from-may-2021.html?m=1
1 )What do you think are the factors in this patient that are contributing to his increased severity of symptoms and infection?
Ans: As the patient has previous past history of :
Type 2 Diabetes Mellitus since 7 years
Chronic Kidney Disease since 2 years
Pulmonary Kochs: 7 years back for which he took 6 months of ATT.
Bronchial Asthma since 7 years
Chronic NSAID use: since 1991 for knee pain
Getting admitted to a Hospital in 2019 for B/L Pneumonia.
These above factors are contributing to his severity of symptoms and infection.
2.Can you explain why the D dimer levels are increasing in this patient?
Ans:The liver produces several important proteins involved in the coagulation process, one of which includes fibrinogen. A single fibrinogen molecule is a symmetrical dimer that is made up of three pairs of three different polypeptide chains, which include a, b and g.
Each of the intertwined polypeptide chains that comprise a single fibrinogen molecule is held together by disulfide bonds.
The formation of fibrin begins with the cleaving of the a and b polypeptide chains of the fibrinogen molecule, which is achieved by thrombin. This cleaving event causes the fibrin monomers to spontaneously polymerize, which results in the formation of double-stranded fibrin protofibrils.
To strengthen a normally weak network that exists between the fibrin monomers and the protofibrils, a transglutaminase enzyme known as factor XIIa is activated.
If an injury occurs, the fibrinolytic system will activate to limit the size of the clot. This system begins with the release of the plasminogen activator from the vascular endothelial cells to allow this molecule to bind to the fibrin surface of plasmin.
Several different studies have looked to measure D-dimer levels in hospitalized COVID-19 patients to determine whether this biomarker could be useful in predicting patient outcomes.
3)What were the treatment options taken up with falling oxygen saturation?
Ans:Failure to initiate oxygen therapy can result in serious harm to the patient. The essence of oxygen therapy is to provide oxygen according to target saturation rate, and to monitor the saturation rate to keep it within target range. The target range (SaO2) for a normal adult is 92 – 98%. For patients with COPD, the target SaO2 range is 88 – 92%
Raise the head of the bed
Deep breathing and coughing techniques
If patient is already on supplemental oxygen, ensure equipment is turned on and set at the required flow rate and is connected to an oxygen supply source. If a portable tank is being used, check the oxygen level in the tank. Ensure the connecting oxygen tubing is not kinked, which could obstruct the flow of oxygen. Feel for the flow of oxygen from the exit ports on the oxygen equipment. In hospitals where medical air and oxygen are used, ensure patient is connected to the oxygen flow port.
Applying nasal prongs
Applying nasal prongs
Oxygen is initially started at a low concentration (2 L/min) using nasal prongs. Then the flow is titrated up to maintain oxygen saturation of 92% or greater.
4) Can you think of an appropriate explanation as to why the patient has developed CKD, 2 years ago? (Note: Despite being on anti diabetic medication, there was no regular monitoring of blood sugar levels and hence no way to know for sure if it was being controlled or not)
Ans : Kidney functions therefore need monitoring at least once per year. Pharmacokinetics of antidiabetic drugs may be altered, once the glomerular filtration rate (GFR) is less than 60 ml/min. Risk of hypoglycemia associated with sulfonylurea and glinide therapies is further increased in the presence of renal impairment. Most sulfonylureas must be discontinued once GFR is <60 ml/min. Some glinides may be continued beyond this threshold, in particular repaglinide, which may be used in dialysis patients. In the absence of co morbidities, metformin can be continued at lower doses until a GFR of 45 ml/min, but must be withdrawn in case of dehydration or co-administration of any nephrotoxic drug including dyes for radiological investigations. Glitazones may worsen water and sodium retention in patients with renal impairment. The pharmacokinetics of all DPP-IV inhibitors are altered with impaired renal function. Only linagliptin may be used in advanced kidney disease, but experience is as yet very limited. GLP-1 agonists are contraindicated in moderate to advanced kidney disease. Lastly, insulin therapy, particularly using the new insulin analogues, allows adequate management of hyperglycemia in chronic kidney disease (CKD) patients, with lower risk of hypoglycemia.
10 ) MEDICAL EDUCATION .
This pandemic presents practical and logistical challenges and concerns for patient safety, recognizing that students
may potentially spread the virus when asymptomatic and may acquire the virus in the course of training. This Viewpoint discusses the current status of medical education, describes how COVID-19 may affect preclerkship and clerkship learniing environments, and explores potential implications of COVID-19 for the future of medical education.
The development of entrustable professional activities and competency-based learning with identified milestones for achievement have transformed assessment.This E log experience enhanced many students to profound into their thoughts and helps in gaining clinical knowledge.





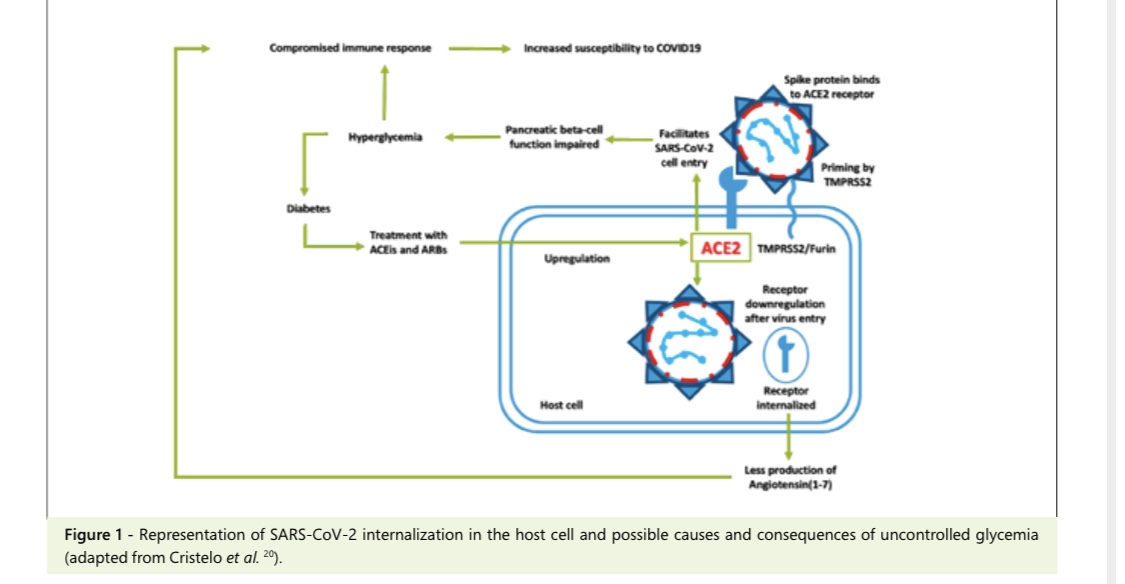 New onset DM in patient may be responsible for late recovery as the virus may thrive in an environment of elevated blood glucose.
New onset DM in patient may be responsible for late recovery as the virus may thrive in an environment of elevated blood glucose.


Comments
Post a Comment